The Clinic for Dermatology & Wellness 2924 Siskiyou Blvd, Suite 200
Medford, OR 97504 Phone: (541) 200-2777 Fax: (541) 214-2575 Tuesday–Friday: 7:30 a.m.–5:30 p.m.
The Annex at the Clinic 2937 Siskiyou Blvd, Suite 1
Medford, OR 97504 Phone: (541) 200-2777 Fax: (541) 214-2575 Tuesday–Friday: 7:30 a.m.–5:30 p.m.
Being diagnosed with skin cancer can bring about a lot of fear and uncertainty. Here’s the good news: You’re not alone, and your treatment options are better than ever. Mohs surgery at The Clinic for Dermatology & Wellness in Medford, Oregon, brings one of today’s most advanced and effective solutions to Grants Pass, Ashland, and Northern California.
Our skilled dermatologists, including fellowship-trained Mohs Surgeon Dr. Anya Bandt, use this highly successful technique to remove skin cancer tumors while preserving as much healthy tissue as possible. On this page, you’ll find answers to all your questions about the approach, from whether it is right for you to what you can expect before, during, and after the procedure.
What Is Mohs Surgery?
Mohs micrographic surgery is a highly specialized surgical technique best suited for certain high-risk skin cancer tumors, as well as for those tumors that have occurred in cosmetically and/or functionally sensitive areas that benefit from minimal excision of tissue.
The surgery is named after innovative American surgeon, Frederic Mohs. The Mohs procedure is widely considered the best treatment for certain types of skin cancers due to its extremely high cure rate while minimizing scarring and loss of healthy skin.
Meet Your Dermatology Team
Our providers are highly trained with extensive academic backgrounds at some of the finest educational institutions in the world. You can trust our board-certified dermatologists to deliver exceptional, innovative care in the Rogue Region.
What Is the Difference Between Mohs Surgery and “Normal” Skin Cancer Surgery?
Mohs surgery is considered the “gold standard” for skin cancer treatment. The main difference between Mohs surgery and other surgical techniques is that it spares as much healthy tissue as possible through a meticulous, staged excision and examination process that typically is performed during a single visit.
During a Routine Excision Skin Cancer Surgery, Your Team Will:
Consider the type of skin cancer and the “stage” or severity (in situ tumor vs. invasive tumor).
Estimate a “margin” (border of unaffected skin around the visible tumor) to help ensure the tumor is completely removed.
Remove the visible tumor, including some of the surrounding tissues, to eliminate all cancerous cells.
During Mohs Skin Cancer Surgery, Your Team Will:
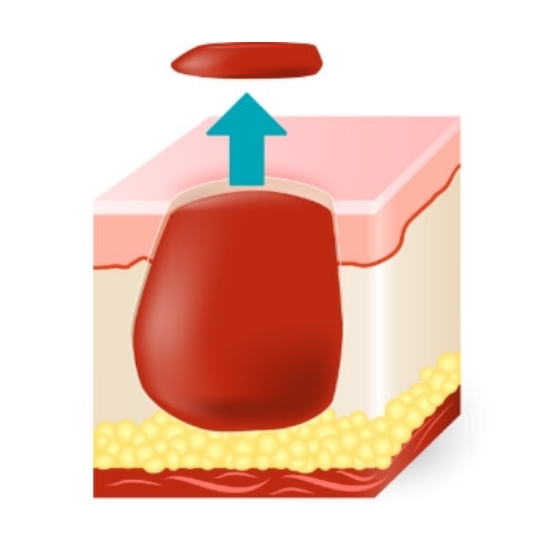
Remove only the thinnest layer of visible cancerous tissue for examination, sparing healthy tissues.
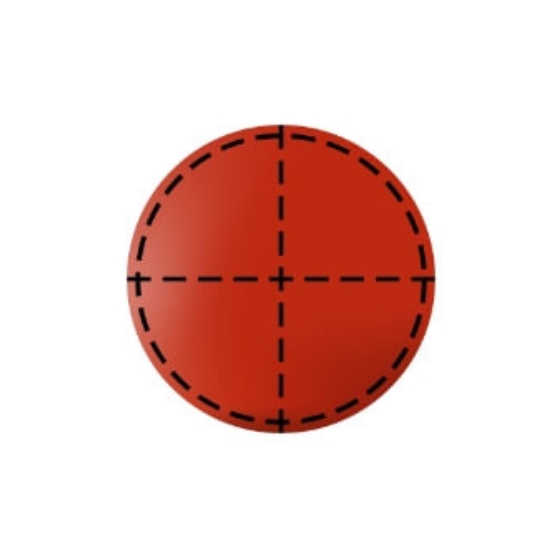
Meticulously “quadrant” and examine the removed tissue margins under a microscope (in “real time”) to determine if any cancer remains.
Continue the process in stages—one tissue layer at a time—until all cancerous tissue is removed.
Alternatives to Mohs Surgery
In addition to traditional surgical excision, alternatives to Mohs surgery include the following:
Photodynamic therapy is best for precancerous actinic keratosis but may be used to treat superficial, early-stage skin cancer.
Your dermatologist will determine the treatment best suited to your specific skin cancer and its location to optimize the success and cosmetic result.
What Are the Benefits of Mohs Surgery for Skin Cancer?
There are several benefits to using the Mohs technique:
Mohs surgery removes all malignant (cancer) cells, including the deeper, root-like cells that traditional surgery may overlook, which are otherwise difficult to see with traditional surgical and pathology evaluation.
Mohs spares the greatest amount of tissue possible from being surgically removed.
Other Benefits Include:
An extremely high cure rate of 98 to 99%
Minimal scarring
Outpatient procedure that typically lasts only several hours
Uses local anesthesia, lowering the risk of general anesthesia or conscious sedation methods.
How Much Does Mohs Surgery Cost in Oregon? Is It Covered by Insurance?
The cost of Mohs surgery at our Medford, Oregon, practice varies from person to person depending on the complexity of the procedure. We will discuss your personalized pricing estimate before your procedure. Most major insurance carriers do cover Mohs surgery for skin cancer treatment.
Am I a Good Candidate for Mohs Surgery?
The use of Mohs surgery is guided by the location, type, and severity of the skin cancer. Mohs is especially ideal in cases when the skin cancer:
Is in an area where it is important to preserve healthy tissue for functional and cosmetic reasons, including the face, scalp, hands, feet, or genitalia
Is large, aggressive, or growing rapidly or uncontrollably
Has recurred (was previously treated and came back)
Has edges or borders that are difficult to determine
Is located on or adjacent to scar tissue
While it is true that Mohs surgery offers the highest rate of success and best cosmetic outcome, not every skin cancer is a candidate for Mohs surgery. Some types of tumors (melanoma in particular) are rarely excised using Mohs surgery. Furthermore, the American Academy of Dermatology and your insurer have guidelines and locations and situations in which Mohs surgery is not recommended.
Ultimately, the type of surgery used for your skin cancer is a discussion between you as the patient and your dermatology team. We will discuss your options and always make a recommendation for the approach that will maximize your best outcome. You can learn more about conditions we treat with Mohs surgery.
Which Types of Skin Cancers Can Be Treated With Mohs Surgery?
Mohs surgery is most commonly used to treat basal cell skin cancer, the most common form of cancer in the United States (4 to 5 million cases annually), as well as squamous cell carcinoma. Other, rarer skin cancer tumors are also eligible for treatment using Mohs surgery.
Basal Cell Carcinoma (BCC)
The most common form of cancer in the United States, basal cell carcinoma is a relatively slow-growing form of cancer that starts in the upper layer of the skin (basal cell layer). BCC rarely spreads to other areas of the body (metastasis).
Squamous Cell Carcinoma (SCC)
Squamous cell carcinoma is the second most common form of skin cancer. SCC has a direct correlation with extensive sun exposure; the most common SCC patient is an older, fair-skinned person with a history of significant sun exposure. SCC rarely spreads. SCC located on the lips and ears, however, do have a known higher risk for metastasis and are always recommended for Mohs surgery here at The Clinic for Dermatology & Wellness.
Dermatofibrosarcoma Protuberans (DFSP)
DFSP is a rare skin tumor of unknown cause. DFSP often presents in early to middle adult life (ages 20 to 55); it is considered to occur in less than 1 in every 100,000 people.
Extramammary Paget’s Disease (EMPD)
EMPD is a rare form of cancer that often resembles a chronic eczema-like rash near the anogenital or axilla (armpits) or both men and women. EMPD has a low mortality rate and is readily treated with Mohs surgery.
Sebaceous Carcinoma
Sebaceous carcinoma is a form of cancer of oil glands that join hair follicles. While sebaceous carcinoma is rare, it is often very aggressive. Mohs surgery is considered the most common and effective form of treatment for this cancer
Microcystic Adnexal Carcinoma (MAC)
MAC is a rare and often slow-growing form of cancer. Often easily treated, failure to successfully treat MAC could result in an invasion of nearby fatty tissues. MAC has a high success rate with Mohs surgery.
What To Expect During Your Mohs Surgery
Mohs surgery is a simple outpatient surgical procedure that uses local anesthesia, so you will not need to be “put under.” This results in a quick surgery with an easier and faster recovery. During your Mohs procedure, you can expect:
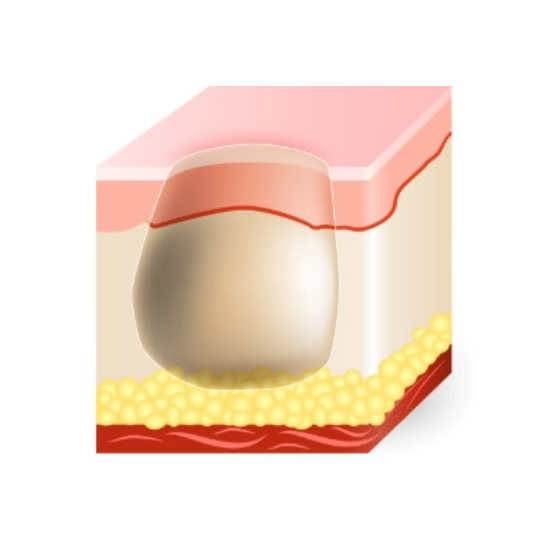
Step 1
Your surgeon will surgically remove the area of the tumor visible to the naked eye.
Step 2
Next, your surgeon will carefully mark the removed tissue in 4 quadrants for reference and the tissue will be processed into slides.
Step 3
Your surgeon will then examine the prepared tissue slides under a microscope and identify each quadrant and area with cancer cells remaining.
Step 4
Steps 2 and 3 are repeated in any quadrant with cancerous tissue. Each iteration of this removal is called a “stage.” The number of stages depends upon the size, location, and aggressiveness of the skin cancer, but most tumors are removed in 1 to 2 stages.
Step 5
Once all cancer tissue has been successfully removed, your surgeon will counsel you about the best technique to repair the surgical site. Some surgeries are best allowed to heal naturally, from the bottom up—this is called secondary intention. Other sites are best repaired with stitches using simple layered closures, or advanced techniques such as flaps or tissue grafts from other locations on the body.
Step 6
Your dermatology provider will work with you to continue skin cancer surveillance by conducting total body skin exams (TBSE) at an interval best designed based on your type of cancer, history of any previous skin cancers, age, and sun exposure history.
What Is Traditional Skin Cancer Excision?
Occasionally, your dermatology provider will recommend a traditional form of skin cancer treatment, simply called surgical excision (removal). This technique is common for simple, non-aggressive tumors on the torso, arms, and legs that do not demonstrate more concerning characteristics. This same procedure (surgical excision) is used on benign lesions such as dysplastic (pre-cancerous) moles, cysts, and benign tumors such as lipomas.
Excisional surgery typically takes an hour from the time of check-in to bandaging the treatment area. While excision requires more healthy tissue to be removed than Mohs surgery, our skilled surgical teams take great care to offer extremely high cure rates while minimizing scarring from the procedure.
How Is Traditional Skin Cancer Excision Performed?
Before your excisional surgery, your surgical team will use local anesthesia to prepare the site and prevent any pain or discomfort during your surgery. Then, your surgeon will:
Outline the visible area of the tumor and create a “margin” of healthy skin to make sure all remnants of skin cancer are removed. Margin size is determined by the type of skin cancer, its aggressiveness, and its location on the body.
Surgically remove the determined area.
Send the excised tissue to the lab for analysis to make sure all remnants of the cancer were fully removed (clear margins). This typically takes a week.
How To Prepare for Your Mohs Surgery
Although Mohs surgery is an outpatient surgical procedure, there are still precautions and steps you can take to maximize your comfort and surgical outcome. We provide the following guidelines to start 2 weeks before your surgery. You can download these guidelines here or obtain them at The Clinic’s front desk.
2 Weeks Before Surgery
We know it’s hard to quit smoking; however, smoking and tobacco use delays wound healing and slows your progress. We ask that you cease nicotine products 2 weeks before surgery.
Unless they are prescribed, we ask that you stop the following medications 2 weeks before surgery as they can cause excessive bleeding:
OK to take if needed: Tylenol, or its generic form, acetaminophen
If you are taking any of the above by prescription, please make sure that the medical staff is aware of your use and the reason to note in your chart and to make sure that the surgeon is aware of your use.
1 Week Before Surgery
It is important to minimize the risk of artificially raised blood pressure during surgery. Therefore, we ask that you discontinue the use of:
Ginkgo biloba
Ginseng
Garlic
Vitamin E
Vitamin C
Fish oil
Other herbal supplements
24 Hours Before Surgery
To protect against raised blood pressure and increased bleeding, we ask that you not drink alcohol, coffee, or any caffeinated beverage at least 24 hours before and after your surgery.
Day of Surgery
On the day of surgery, we ask that you:
Please bathe (shower or bath) and ensure that you wash the area of the surgery and your hair.
Do not use any makeup if your skin cancer is on the face.
Make sure to take all scheduled, prescribed medications (unless otherwise directed by our medical staff), including blood pressure, diabetes, and cholesterol drugs. We also ask you to bring 1 day’s supply with you to your surgery.
We will have light snacks and drinks available; you should be prepared to spend at least 3 to 4 hours through the morning or early afternoon. Please bring a book, iPad, or something to occupy your time.
Mohs Surgery Recovery & Aftercare
We request that a family member or friend accompany you on the day of your surgery to provide companionship and to assist you in getting home. Do not make important plans in the days immediately following your surgery.
Many people are concerned about pain after their Mohs surgery; however, for the great majority of patients, postoperative pain is very mild and rarely needs medications beyond Tylenol (acetaminophen).
How Long Do Swelling & Bruising Last After Mohs Surgery?
Swelling and bruising are common following Mohs surgery, particularly when surgery is performed around the eyes. This usually occurs within 5 to 7 days after surgery and may be decreased by using an ice pack during the first 24 to 48 hours.
Please keep in mind that it often takes months before final wound healing is complete, and the best cosmetic result is obtained.
Are There Any Activity Restrictions After Mohs Surgery?
Although rare, bleeding after surgery is the most common potential postoperative complication. To minimize the chances of this occurring, please reduce activity as much as possible after surgery—no bending, heavy lifting, vigorous exercise, or exertion. You will receive specific aftercare instructions based on your surgical site, including a timeline for resuming daily activities and exercise.
What Are Possible Side Effects I Should Know About?
Infection is also a possibility following surgery, but it occurs only in 1 to 2% of patients. Often a small red area may develop surrounding your wound. This is normal and does not necessarily indicate infection. However, if this redness does not subside, and if the wound begins to drain pus or becomes swollen or very tender, you should notify us immediately.
At times, the area surrounding your wound will be numb to the touch. This may persist for weeks or months and, in some instances, can be permanent. This is due to trauma to the small nerve endings on the skin surface that occurs during the removal of the tumor.
The best alternative to Mohs surgery depends on multiple factors, including the type and location of the cancer, which treatments have already been tried, and individual patient preferences.
What is the average age for Mohs surgery?
The average age for a Mohs skin cancer surgery patient is around 65. Because sun exposure accumulates over the years, non-melanoma skin cancers, such as basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), are most common in older adults. However, Mohs surgery is performed on patients across a wide age range, including younger individuals, especially those with risk factors such as having lighter skin, hair, and eyes, a genetic predisposition, or immune suppression.
Do they put you to sleep for Mohs surgery?
No, we do not use general anesthetic for Mohs surgery. We typically perform the procedure using a local anesthetic, which numbs the area but allows you to remain awake and alert.
How painful is a Mohs procedure?
Mohs surgery is performed under local anesthesia, so you shouldn’t feel any pain. Some patients report feeling pressure or mild discomfort while the surgeon works. After the surgery, the surgical site may be sore or tender, but discomfort is typically manageable with over-the-counter pain relievers.
Can I drive home after the procedure?
We require that Mohs patients have a trusted adult bring them to the surgery and stay to provide support and a safe ride home.
How many hours does Mohs surgery take?
The average surgery takes 3 to 4 hours. Because Mohs surgery is an iterative process, we ask that patients prepare to spend the whole day with us.
What does a Mohs scar look like?
Mohs surgery scars vary with the size and location of the skin cancer. They are initially pink or red and raised but typically fade over time, becoming less noticeable. Your surgeon will give you aftercare instructions to minimize scarring; in some cases, reconstructive techniques can further improve the appearance of the scar.
Will I need plastic surgery after Mohs surgery?
Depending on the size and location of the cancer, some patients may benefit from reconstructive surgery after Mohs to improve the cosmetic outcome, especially if the surgery leaves a significant scar or is on the face. Our Mohs surgeons are skilled in minimizing scarring and performing basic reconstruction at the time of the procedure.
Should I be nervous about Mohs surgery?
Feeling apprehensive before a medical procedure is normal, but keep in mind that the surgical area will be numb. Mohs surgery is a highly precise procedure that preserves as much healthy tissue as possible. It has a very high cure rate. Your dermatologist will walk you through the process to help ease any of your concerns.
Your Healthiest Skin Starts Today
Receiving a skin cancer diagnosis is a stressful experience, but rest assured you have an experienced team that is on your side and ready to help. If you would like to discuss your treatment options with one of our trained Mohs surgeons please book online or call
(541) 200-2777. We look forward to helping our Medford Mohs patients from Ashland and throughout Southern Oregon enjoy the beauty of healthy skin.
Take Control of Your Health with an Annual Skin Exam
When it comes to skin cancer, time is of the essence. The sooner potential issues are identified, the higher the likelihood of successful treatment. Yearly skin cancer screenings are the cornerstone of early detection, enabling us to identify any warning signs and act quickly. Think of your annual skin exam as your proactive step toward a lifetime of skin health.








{kind=link}